by Evan Blauser
Medicaid News Update
On February 4, 2019, the Wyoming House of Representatives failed to pass HB 244, an act that would have expanded Medicaid to able-bodied, working-age adults making 138% of the Federal Poverty Level (FPL). The action taken by the House could potentially save the state of Wyoming $17 million per year.
Wyoming spends an average of $6,466 per Medicaid enrollee, and it is estimated that an additional 27,000 individuals would be eligible for enrollment after expansion. So the approximate cost of expansion would be $6,466 x 27,000 = $17 Million (after accounting for the fact that Wyoming would only pay for 10% of expansion). The Wyoming Liberty Group applauds the actions of the House of Representatives, and we hope people in Wyoming will make the right choice if a ballot initiative is proposed.
What happens now?
The Wyoming legislature now wants to conduct a $150,000 study into the cost of Medicaid expansion, despite the fact that numerous studies and research have been conducted to determine what costs would be associated with expansion. Prior to HB 244 being struck down, the Wyoming Liberty Group conducted an exhaustive study into the viability of Medicaid expansion, and how it could effect the state of Wyoming.
This research included several items listed in Senate File 146, the Medicaid expansion cost study bill. Namely, our research examined the effects of expansion in several surrounding states, we studied the financial impact on Wyoming, and we looked into who exactly would receive benefits under expansion (the primary beneficiaries would be able-bodied, working-age adults making 138% of the Federal Poverty Level).
In order to save the state of Wyoming $260,000 ($150,000 for the initial study, plus an additional $110,000 for a new employee to conduct the study), the Wyoming Liberty Group recommends using our research, in conjunction with the multitude of other studies, to determine whether expansion would be financially viable in Wyoming. After a careful reading of our analysis, we trust that legislators and the public will have a better understanding of the damage presented by Medicaid expansion.
On March 23, 2010, President Barack Obama signed the Patient Protection and Affordable Care Act into law. This established an avenue for the 50 states to expand Medicaid to able-bodied, working-age adults making 138% of the Federal Poverty Level. Fortunately, the Supreme Court ensured that states would not be forced to expand Medicaid, and could instead choose for themselves. Following this victory for states’ rights, all but nine of the states have expanded Medicaid. Nebraska, Idaho, and Utah recently passed expansion through a ballot initiative supported by out-of-state forces. These same influencers are looking to expand Medicaid in Wyoming, Texas, and the remaining seven hold outs. In this fact sheet, the Wyoming Liberty Group hopes to better inform the public about several significant issues associated with expanding Medicaid coverage to able-bodied adults.
First, we will examine the positive effects of not expanding Medicaid, namely by calculating exactly how much money the state of Wyoming has saved since the option of expansion was first presented in 2014. Next, we will explore the detrimental economic costs associated with expanding coverage to able-bodied individuals. Our research indicates that expansion states have seen higher enrollment numbers than expected, which has resulted in states footing a larger portion of the bill than they accounted for. Then we will discuss the impossibility of the government keeping their promise to cover 90% of state costs for the remainder of the Medicaid program. We will look at the human impact of Medicaid expansion, which is that truly needy individuals (blind, elderly, disabled, and low-income populations) are being squeezed out of coverage to support the newly-enrolled, able-bodied adults.
Finally, we offer alternative solutions to Medicaid coverage, ranging from insurance pools to direct pay solutions. The goal of this fact sheet is to put forth the argument that Wyoming would not be “missing out” on federal money by not expanding, and would instead save tax dollars and lives by keeping coverage for the truly needy in our beautiful state.
I. How much would Wyoming save by not expanding Medicaid coverage to people making 138% of the Federal Poverty Level?
- Healthinsurance.org estimated that there are approximately 27,000 people who could be eligible for Medicaid if it were expanded (it should be noted that the only reason that they are currently not covered is because they are childless, working-age adults). Given that the average per-enrollee spending in Wyoming is $6,466, the yearly savings of not insuring these individuals comes out to $17,458,200. That means that our total Medicaid savings over the next 5 years would be $87,291,000. Of course, this projection was made assuming that Wyoming would eventually pay 10% of the costs of Medicaid. Keep in mind, that’s just what we saved on Medicaid expansion alone, and that our total Medicaid budget would have been eclipsed by the money we would have spent on expansion. Not only that, but due to a miscalculation by state governments, more people than expected have signed up in nearly every state that expanded Medicaid. So, that $87 million was the low end estimate, and the real number would likely be higher.
- Prior to discussing the total Medicaid budgets of the surrounding states, it is necessary to account for the per-enrollee spending of the states in question. This is done to ensure fairness in our analysis. The per enrollee spending of Nebraska, Utah, Idaho, Montana, Colorado, and South Dakota are below, along with Texas, Florida, Ohio, New York, and California. These last few states are the biggest spenders in Medicaid, something we will discuss at length:
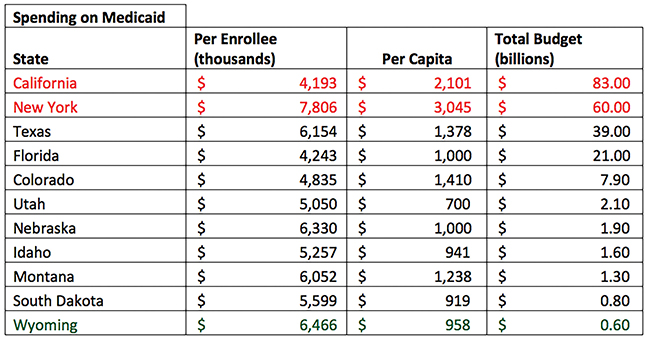
- Even when you account for their larger population sizes, California and New York still spend dramatically more per capita than do the other states examined in this report. That can only mean that these larger states aren’t spending more money because of their size, they are spending more money because they had too many people enroll in their Medicaid programs.
- You should keep in mind that the only states with less than $1 billion in their Medicaid budgets are Wyoming and South Dakota, two states that have yet to pass Medicaid expansion. In contrast, early adopters of Medicaid (California and New York for example) have seen their budgets explode. For instance, California’s Medicaid budget in 2002 was $27.2 billion, and it currently sits at a whopping $83 billion. By comparison, New York’s Medicaid spending amounted to $44.5 billion in 2012, and has sharply increased since then. The larger states should be spending more on Medicaid, because they have more people. However, when you examine the total percentage that Medicaid swallows up in their budgets, it is clear that expansion has significantly diminished the states’ ability to keep up with other spending priorities. California, for example, saw their state budget increase from 18.9% in 2012 to 33.5% in 2016. That means that for every dollar that the state of California spends, 33.5 cents goes directly to pay for Medicaid. Meanwhile, Wyoming’s Medicaid budget has remained relatively flat during the period of expansion.
- Unfortunately, Healthinsurance.org continues to perpetuate the myth that Wyoming would be “leaving money on the table” if we refused to expand Medicaid. This could not be further from the truth. While they are correct when they say that the federal government would pay for the majority of expansion, they fail to recognize the threat to the overall state Medicaid budget. These are not “free” federal funds that could be used to improve Wyoming. Instead, these funds would only be used to cover medical insurance for able-bodied, working-age, childless adults making 138% of the Federal Poverty Level, or $34,638 a year for a family of four. Make no mistake, this is not a federal investment plan to improve the state of Wyoming, this is an avenue for the federal government to take control of our lives by making healthcare the governments’ responsibility. We have to ask ourselves whether we are willing to forfeit some of our state sovereignty in order to have partially subsidized healthcare. The Wyoming Liberty Group is not, nor will we ever be, prepared to make such a concession to the federal government.
II. What happened in expansion states?
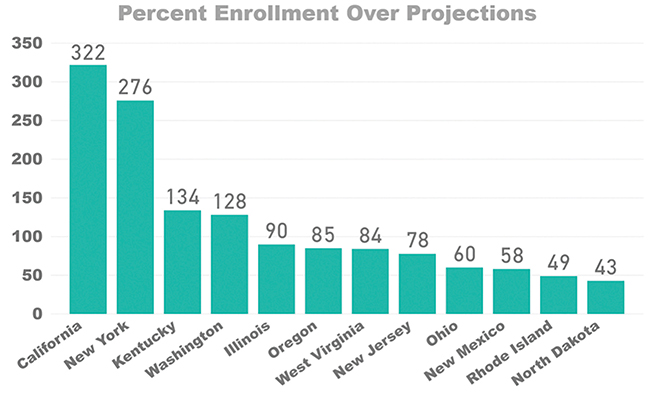
- When California expanded Medicaid, they predicted an additional 910,000 people would enroll. Instead, 3.8 million people signed up for Medicaid, which cost the state $43.7 billion in the first 3 years of Medicaid expansion.
- According to the Foundation for Government Accountability (FGA) Obamacare expansion states have enrolled twice as many people than they initially projected. Here is a graph demonstrating the “woodwork effect” that happens as more Americans are compelled to enroll in government subsidized healthcare, instead of seeking healthcare through alternative measures (discussed at length at the end of this report).
 Source: link
Source: link
Raw data for Projected/Actual Enrollment:
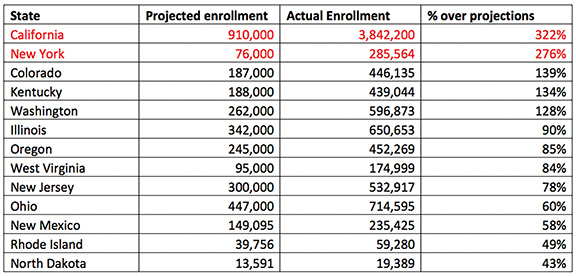
- As you can see, the several states that have expanded Medicaid coverage to able-bodied adults have seen enrollment surpass the federal government’s wildest imaginations. This is just a snapshot of a national miscalculation on the part of the government, with the combined numbers for 2016 coming out to a predicted 5,452,842 enrollees, and an actual enrollment of 11,466,254 enrollees.
- Now take the national average miscalculation, and apply it to Wyoming to see what we could potentially be spending on Medicaid expansion in the real world. The national average under projection was 110%, which applied to our projected expansion population would mean that an additional 2,700 individuals would be enrolled in Wyoming, costing the state another $17,458,200 (2,700 x $6,466) in the first year alone.
- Of course, we have to take into account that the federal government has promised that it will pay up to 90% of the costs of expansion in the foreseeable future, which brings me to my next point.
III. What happens if the federal government cannot keep their 90% promise?
- In 2015, shortly after states started expanding Medicaid coverage to individuals making 138% of the Federal Poverty Line, the United States spent $545 billion on Medicaid, which made up almost 10% of the federal budget in that year. Since 2015 the national Medicaid budget has soared to $581.9 billion, or 17% of the National Health Expenditure of the United States (the NHE takes into account all of the healthcare spending in the U.S., including Medicare, Medicaid, private health insurance, out of pocket expenditures, prescriptions, etc.). According to the Centers for Medicare & Medicaid Services (CMS), the NHE grew 3.9% between 2016 and 2017, to a total of $3.5 trillion or 17.9% of the total Gross Domestic Product (GDP). State and local governments were on the hook for 17.1% of the total NHE in Fiscal Year 2017, while the federal government paid for 28.1% of total NHE expenditures.
- Now let us take a look at the projections from the CMS, keeping in mind that they are the low-end projections for national healthcare spending. They estimated that total NHE spending will increase at an average rate of 5.5% per year between 2017 and 2026, amounting to a total of $5.7 trillion by 2026. What is more, they projected that healthcare spending will outpace GDP growth by an average of 1.0% per year, meaning that the health share of GDP will increase to 19.7% of GDP by the year 2026.
- Keep in mind that this is mandatory spending, meaning that before the U.S. government spends a dime on improving roads or increasing teachers’ salaries, we will have to pay for our Medicaid debt. With a total national debt of $21 trillion last year, the sustainability of Medicaid is in serious doubt. What happens when the national government fails to foot their promised 90% of the expansion bill? We, the states, will have to increase taxes in order to pay off our debts to doctors, nurses, hospitals, and pharmaceutical companies. In the meantime, let us talk about what increasing the number of enrollees in Medicaid will do to the truly needy people of Wyoming: the blind, elderly, disabled, or low-income individuals who are already covered under Medicaid.
IV. Unintended consequences of expanding Medicaid coverage to able-bodied adults.
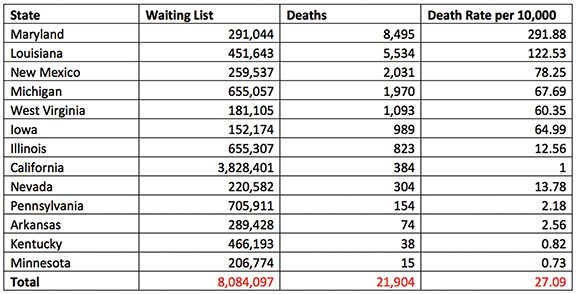
- Following Medicaid expansion, more than 28 million able-bodied adults across the United States were able to enroll in Obamacare. The result of this expansion of coverage was that nearly 250,000 truly needy individuals were placed on the Medicaid waiting list, which means that they were unable to receive the care they desperately needed. The reason this happens is simple: if more and more able-bodied adults are flooding the Medicaid market, then that means there are fewer resources to be distributed amongst the truly needy people for whom Medicaid was created.
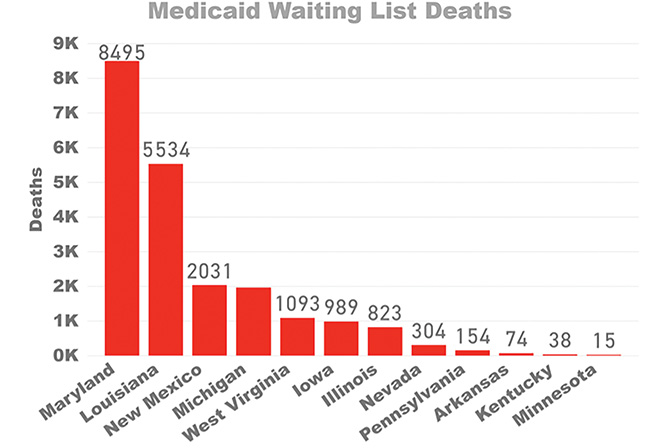
- What happens to the people on Medicaid waiting lists? According to a blistering report put out by the Foundation for Government Accountability (FGA), since Obamacare expansion took effect, more than 21,000 truly needy Americans have died because they were on a Medicaid waiting list. This is the human impact that expansion could have as a result of the concerning numbers mentioned earlier. Here is a full list of the waiting list deaths, provided by the FGA:
Source: link
Demonstrated in the graph above: “Crowding out” effect that happens when the government allows able-bodied adults to enroll in Medicaid.
Raw data from the Foundation for Government Accountability:
- The economic impact of Medicaid expansion goes beyond state and federal budget deficits, and will eventually reach every taxpayer in every expansion state in the nation. The simple truth of the matter is that states that expand Medicaid will eventually have to rely on their citizens to pay the state portion of the bill. Unfortunately for doctors and nurses, some states have already started looking at them to empty their coffers.
- Some key examples are in Oregon, one of the first states to expand Medicaid in 2012, Indiana, Ohio, and Illinois. These states have started to implement what is known as “provider taxes” to pay for the states’ share of Medicaid. You read that right, in an effort to provide low-income individuals medical care, states are starting to tax medical providers (doctors, nurses, hospitals, etc.). According to the Council of State Governments (CSG), every state except for Alaska now has these provider taxes in place, setting the scene for a backwards tax-and-spend formula that will inadvertently drive the cost of healthcare up in states that already cannot afford it. Ask yourself if it would make sense to pay for Supplemental Nutrition Assistance Program (SNAP) benefits by taxing grocery stores that provide the food to needy individuals.
- One recent example of an increase in taxes is in Montana, which passed Medicaid expansion, but failed to pass a tax on tobacco products to pay for expansion. Let this be a lesson to every Wyomingite: if the state passes expansion, we will be the ones to pay for it.
- Perhaps the best method to understand the detrimental effects that Medicaid has had on states that sought expansion is to examine the percent of their budgets that Medicaid encompasses. Here is a map that demonstrates the damage that miscalculations can cause. You will notice that the states with the highest percent of their budgets dedicated to Medicaid are those with higher enrollment numbers (again California and New York stand out with 34.3% and 32.6% Medicaid spending respectively). Wyoming, South Dakota, and Nebraska are at the lower end of the spectrum, with 13.9%, 21.1%, and 17.5% being spent on Medicaid in the states. Common sense tells us that when Medicaid eats away more of the budget, other spending priorities like the Fire Department, Police, roadways, and education are pushed aside so the state can afford to pay for its Medicaid population.
- To drive this point home, consider Milton Friedman’s position on the issue of higher taxes, “nobody spends somebody else’s money as wisely as he spends his own.” Do you really want to be on the hook for the federal government’s Medicaid mistakes?
V. Alternatives to Medicaid
- You may be asking yourself, if we do not endorse Medicaid expansion, then what do we support? I am glad you asked, as there are multiple alternative options for low-income individuals seeking medical coverage. First and foremost, there are section 1115 Medicaid demonstration waivers that would allow the Secretary of Health and Human Services (HHS) to waive provisions of major healthcare legislation in order to allow states to avoid expanding Medicaid entirely. This is the option that I hope Wyoming decides to take in lieu of expansion. The Section 1115 waivers also allow the states to allocate Medicaid dollars in any health-related fashion, meaning that states could invest in more affordable coverage plans for low-income individuals.
- Following the 1115 waiver, our state would have several options to providing healthcare to individuals at or below the 138% Federal Poverty Level threshold. These options include insurance pools, direct-pay to doctors, and, if Congress would allow it, the ability to buy health insurance across state lines. In order to understand what a health insurance pool is, let us look at high-risk pools. Prior to the Affordable Care Act’s passage, most insurance companies would not cover individuals with “pre-existing conditions” like heart disease and diabetes. Now, state governments offer what they call “high-risk pools” for people with pre-existing conditions. Although high-risk pool premiums can be double that of a traditional coverage plan, the idea of pooling groups of people together to more easily afford coverage holds true for those on the brink of poverty.
- These short term plans demonstrate the plans offered to a family of four making $34,000 per year, with no smokers or serious health concerns. As you can see, several of the plans offered are affordable, with prices as low as $72.41 per month. I was able to “sign-up” for these plans by going through Wyoming’s healthcare exchange market-place.
- Currently, you are not allowed to buy health insurance across state lines, meaning that a competing healthcare company in Colorado cannot provide the same product at a reduced price to Wyomingites. If this were to change, then healthcare could become a more competitive enterprise, lowering the cost of insurance and benefiting consumers in the long-run. With the signing of an executive order on October 12, 2017, President Donald Trump opened a path for Association Healthcare Plans to take effect. Hopefully, the full scope of this new policy comes into effect and allows individuals to purchase healthcare across state lines.
- Of course, simpler plans often turn out to be more cost effect. What could be simpler than visiting your doctor and paying them directly for the care you received? This is the philosophy of the Direct Primary Care Coalition, which offers healthcare access (instead of coverage) for as little as $70 per month. In return you can visit your doctor without third-party billing, premiums, or insurance of any kind. Currently there are two medical facilities that offer direct pay access to Wyomingites:
307 HEALTH 250 N. Evarts St. • Powell, WY 82435 • www.307health.org
MOUNTAIN SAGE FAMILY CLINIC 1428 Warm Springs Dr • Dubois, WY 82513
link - All of these alternative methods for gaining access to healthcare allow the individual to determine their own medical fate, and hopefully more physicians will start to realize that offering direct pay care, or another option to low-income individuals, will save money for everyone in the long run.
In conclusion, the arguments against expanding Medicaid are simple and make fiscal sense:
- We have saved at least $87 million for the state of Wyoming since not expanding in 2014.
- In nearly every expansion state, enrollment has far outpaced projections, which ends up costing taxpayers more money in the long run.
- By adding able-bodied, working-age adults to Medicaid, we are squeezing out truly needy individuals for whom Medicaid was created.
- Wyoming would not be “missing out” on Medicaid dollars, because that money would not be an investment in Wyoming from the federal government. Instead expansion would end up costing Wyoming taxpayers millions of dollars (which is why Montana tried to pass a tax increase on tobacco to pay for expansion).
- Right now, there are multiple avenues for low-income, working-age adults to have health insurance. If we invest in these alternatives, then we can make private healthcare more affordable.
